
5 Essential Tips for Successful Tibial Plateau Fracture Recovery
A tibial plateau fracture turns life upside down very suddenly. Walking, driving, working, and even sleeping can feel difficult overnight. You may worry about surgery, long rehab, and whether your knee will ever feel “normal” again.
Recovery is absolutely possible. Many people return to work, sports, and active lifestyles after this type of knee injury. The journey just takes time, structure, and a clear plan.
This guide walks you through five essential tips for healing your knee, understanding your surgery or brace, and avoiding setbacks. You will also learn what doctors look for on imaging, which complications matter most, and how to protect your long‑term joint health. 💪
Tip 1: Understand Your Tibial Plateau Fracture and Your Knee 🦴
Feeling informed is one of the best ways to reduce anxiety and stay engaged in recovery. Let’s start with what this injury means and why your care team is being so careful.
What is the tibial plateau?
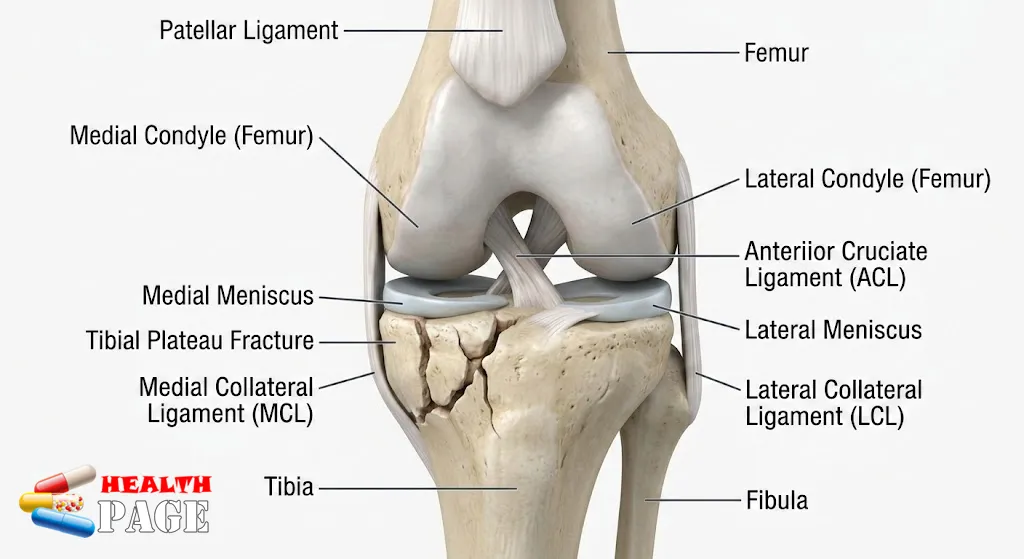
The tibial plateau is the top part of your shinbone (tibia) where it meets the thighbone (femur) to form the knee joint.
It has two main parts:
- Medial condyle (inner side)
- Bears about 60% of your knee load
- Has a concave shape and stronger bone
- Lateral condyle (outer side)
- Bears about 40% of your knee load
- Has a convex shape and relatively weaker bone
Other key structures around the plateau:
- Menisci (medial and lateral)
- Act as shock absorbers and stabilizers
- Lateral meniscus is more mobile
- Ligaments
- ACL, PCL, MCL, LCL all help keep the knee stable
- Normal range of motion (ROM)
- Roughly 0–140°
- Everyday walking usually needs 0–70°
When this joint surface breaks, it can damage bone, cartilage, ligaments, and menisci together. That is why this injury feels so complex.
How common is this injury?
Tibial plateau fractures are not rare, but they are not everyday sprains either:
- Around 10.3 per 100,000 people each year
- About 1–2% of all fractures
- Average age around 52 years
- Two common age patterns:
- Men in their 40s after high‑energy trauma
(motor vehicle crashes, sports accidents, falls from height) - Women in their 70s after low‑energy falls
(often linked with osteoporosis)
- Men in their 40s after high‑energy trauma
Where do these fractures usually happen?
The fracture pattern depends on the direction of the force:
- Lateral plateau (outer side): 70–80%
- Often from a valgus force (knee pushed inward)
- Medial plateau (inner side): 10–20%
- Often from a varus force (knee pushed outward)
- Bicondylar fractures (both sides): 10–30%
- Often from axial loading (strong direct compression, such as falls from height)
Understanding fracture types: The Schatzker system
Doctors often describe the fracture using the Schatzker classification. It sounds technical, but it helps guide treatment and surgery planning.
| Schatzker Type | Main Pattern | Key Clinical Notes |
|---|---|---|
| I | Lateral split | Young, strong bone; often high‑energy |
| II | Split + depression | Most common; lateral meniscus often at risk |
| III | Pure depression | Often elderly, osteoporotic bone |
| IV | Medial plateau | Higher risk of neurovascular injury |
| V | Bicondylar | Both condyles broken; tibial spines still attached |
| VI | Metaphyseal‑diaphyseal dissociation | Severe soft tissue damage; unstable knee |
Some surgeons also use:
- Hohl & Moore classification for fracture‑dislocations
- 3‑column concept (medial, lateral, posterior) to plan fixation strategies
You do not need to memorize all this. But having a rough idea of your fracture type helps you ask focused questions and follow your plan more confidently. 😊
Why are associated injuries so important?
A fracture here often comes with other damage:
- Meniscal tears
- Especially the lateral meniscus
- More common when the joint surface is depressed more than 10 mm
- ACL injuries
- Seen often in Schatzker IV and VI patterns
- Roughly 25% of these more complex cases
- Compartment syndrome
- Swelling and bleeding increase pressure in the lower leg compartments
- Occurs in 7–20% of cases
- Requires emergency fasciotomy to save muscle and nerve function
- Neurovascular injury
- Risk is highest with fracture‑dislocations
- Especially in some type IV (medial) injuries
Knowing these risks explains why your team is checking pulses, sensation, swelling, and pain so closely, especially in the first days.
Tip 2: Get the Right Diagnosis and Treatment Plan 🏥
Accurate imaging and careful planning are crucial. A fracture of the tibial plateau is not a “one size fits all” injury. Treatment depends on displacement, stability, soft tissue condition, and your overall health.
Step 1: Imaging and diagnosis
Most patients go through a staged imaging pathway:
- X‑rays (radiographs)
- Standard views: AP (front), lateral (side), and oblique
- Sometimes a special plateau view to see the joint surface better
- CT scan
- Almost always used for surgical planning
- Shows the degree of depression, comminution (many small fragments), and posterior involvement
- MRI
- Helps detect meniscal tears, ligament injuries, or occult fractures
- Often done when soft tissue damage is suspected or symptoms persist
You can ask your surgeon to walk you through your images. Seeing them can make the plan feel more logical and less mysterious.
Step 2: Nonoperative vs operative treatment
Not every case needs surgery. Treatment choices usually fall into three categories.
1. Nonoperative treatment
Suitable for:
- Minimally displaced, stable fractures
- People who are nonambulatory or have severe medical risks
- Some elderly patients with low‑demand lifestyles
Options include:
- PTB (patellar tendon bearing) cast
- Knee immobilizer
- Hinged knee brace set to limited ROM
You will still need:
- Pain control
- DVT prevention strategies
- Guided physical therapy
- Careful follow‑up X‑rays to confirm the joint surface stays aligned
2. Operative treatment (ORIF)
Open reduction and internal fixation (ORIF) is common when:
- Depression is more than 5–10 mm
- Joint widening is more than 5 mm
- Instability is more than 10°
- The fracture involves the medial side or is bicondylar
Surgery timing can be:
- Early (acute)
- If swelling is mild and skin condition is acceptable
- Staged
- Temporary external fixation first, to protect soft tissues
- Definitive ORIF when swelling improves
Typical surgical tools and steps:
- Approaches: anterolateral, posteromedial, or combined
- Bone grafting:
- Autograft (your bone)
- Allograft (donor bone)
- Synthetic bone substitutes
- Plates and screws:
- Locking plates, buttress plates, and “raft screws” to support the joint surface
For a deeper technical overview of injury patterns and fixation, many surgeons refer to resources.
3. Primary arthroplasty in selected patients
In some patients over 65 years with very osteoporotic bone, heavy joint damage, or pre‑existing arthritis, surgeons may consider:
- Primary knee arthroplasty (knee replacement) instead of ORIF
This is not common in younger or active patients, but can be the most functional option in fragile bone.
Your role in the treatment decision
You and your care team should discuss:
- Your age and activity level
- Your job demands and caregiving roles
- Past knee injuries or arthritis
- Medical conditions that may affect healing
(diabetes, smoking, vascular disease, osteoporosis)
Ask direct questions:
- “What are the pros and cons of surgery for my specific fracture?”
- “What does my recovery look like month by month?”
- “How will we protect my soft tissues and joint surface?”
Feeling heard and informed sets the stage for better cooperation and better results.
Tip 3: Protect the Repair While Staying Safely Active 🚶♀️
After you leave the hospital, the main goals are:
- Protect the fracture or fixation so it can heal
- Prevent stiffness, weakness, and clots through safe movement
Striking this balance is key.
Weight‑bearing: Follow the plan exactly
Most patients start with non‑weightbearing (NWB) or toe‑touch weightbearing (TTWB) for several weeks. The exact timeline depends on:
- Fracture type and complexity
- Quality of fixation
- Bone quality (osteoporotic vs strong)
- Your pain and soft tissue healing
Your surgeon might progress you to:
- Partial weightbearing (PWB) after X‑ray or CT checks
- Full weightbearing (FWB) when the fracture shows solid healing
Trying to walk fully too early risks loss of reduction (5–30% incidence). That can lead to malalignment and arthritis later. On the other hand, staying too inactive increases stiffness, DVT, and muscle wasting.
Use your walker, crutches, or frame as instructed. It is not a sign of weakness. It is a temporary tool to protect your knee. 💡
Bracing and positioning
You may have:
- A hinged knee brace
- Early on, it may be locked in extension during standing
- ROM may be gradually increased for sitting and exercises
- A knee immobilizer or cast for nonoperative cases
General positioning advice (always confirm with your team):
- Keep the leg elevated above heart level to reduce swelling
- Avoid long periods with knee fully flexed in a chair
- Change positions regularly to avoid stiffness and pressure injuries
Safe early movement
Even while non‑weightbearing, you will often be encouraged to:
- Perform ankle pumps and quadriceps sets
- Start assisted knee ROM, usually aiming toward 0–70° for functional walking later
- Do hip and core exercises to maintain general strength
Your physical therapist will guide:
- How far to bend
- Which exercises are allowed
- How many repetitions and sets
Report any sudden increase in pain, popping, or new deformity immediately. It may signal a hardware problem or shifting of the fracture.

Tip 4: Commit to a Structured Rehabilitation Program 🧘♂️
Rehabilitation is where you regain function, not just heal bone. Many people underestimate this stage. Consistent physiotherapy can be the difference between a stiff, painful knee and a strong, functional one.
Why rehab matters so much
Common long‑term issues after this injury include:
- Knee stiffness in 10–25% of patients
- Especially in bicondylar fractures and long immobilization
- Post‑traumatic arthritis in 25–35%
- About 3–7% may need a total knee arthroplasty after 10+ years
Effort in rehab cannot erase all risk, but it can reduce stiffness, improve ROM, and support joint alignment.
Typical phases of rehab (timelines vary)
Always follow your surgeon and therapist’s specific instructions. The outline below is only a general pattern.
Early phase (Weeks 0–6)
Goals:
- Control pain and swelling
- Protect fracture / hardware
- Begin gentle ROM and muscle activation
Common elements:
- Ice, elevation, compression
- Ankle pumps, quadriceps sets, glute squeezes
- Assisted knee flexion and extension within allowed limits
- Gait training with crutches or walker
Middle phase (Weeks 6–12+)
Goals:
- Increase ROM, aiming toward 10–120° or more
- Begin closed‑chain strengthening when safe weightbearing is allowed
- Improve balance and gait pattern
Common elements:
- Stationary bike (no resistance initially)
- Leg presses within limited range
- Step‑ups, mini squats (once cleared)
- Balance work on stable and then unstable surfaces
Late phase (3–9+ months)
Goals:
- Restore near‑normal leg strength and endurance
- Improve agility for work and recreation
- Prepare for sport‑specific or job‑specific tasks
Common elements:
- Progressive strengthening (machines, free weights, bands)
- Treadmill or outdoor walking, then light jog when permitted
- Lateral movements, low jumps, and cutting drills for athletes
Be honest with your therapist
Tell your physiotherapist about:
- Any sharp pain, catching, or giving way
- Fear or anxiety about certain movements
- Work demands you need to return to
- Hobbies you hope to resume (hiking, cycling, gardening, etc.)
Together, you can design a realistic plan that builds confidence as well as strength.
Tip 5: Watch for Complications and Plan for the Long Term 🔍
Recovery from a complex knee fracture is a marathon, not a sprint. Being aware of possible problems helps you act early and protect your future mobility.
Short‑term complications to watch for
Seek urgent care if you notice any of the following.
1. Compartment syndrome
This is rare but serious. It usually occurs in the first days after injury or surgery.
Red flags:
- Severe, increasing pain not relieved by medication
- Pain with passive stretching of the toes or ankle
- Numbness, tingling, or a sense of tightness in the leg
- Skin that feels very tense or “wood‑like”
This condition requires emergency fasciotomy to release pressure and save tissue.
2. Infection
Reported rates are around 2–11%, higher with:
- Open fractures
- Long or complex surgeries
- Poor soft tissue coverage
Watch for:
- Redness, warmth, or drainage at the incision
- Fever or chills
- Increasing pain or swelling at the surgical site
Prompt antibiotics and sometimes further surgery may be required.
3. Deep vein thrombosis (DVT)
DVT occurs in about 6–9% of patients after this injury.
Signs include:
- Swelling in the calf or thigh
- Warmth or redness in one leg
- New, unexplained pain in the leg
Shortness of breath or chest pain can signal a pulmonary embolism and require emergency care.
Longer‑term issues and their impact
Post‑traumatic arthritis
Because the injury affects the joint surface, arthritis is a real risk:
- Occurs in 25–35% of patients long term
- 3–7% may eventually need a total knee replacement
Maintaining healthy weight, strong muscles, and good alignment can ease symptoms and delay progression.
Nonunion and malunion
- Occur in 2–4% of cases overall
- Higher risk in severe Schatzker VI patterns
Symptoms can include persistent pain, deformity, and difficulty weightbearing. Some cases require corrective surgery.
Knee stiffness and functional limits
Even with perfect healing on X‑ray, some people have:
- Trouble kneeling or squatting
- Discomfort on stairs or uneven ground
- Reduced ROM despite therapy
The average ROM after one year is around 10–145°. That is functional for most daily activities, but it may not match your pre‑injury knee.
Return to work and life
Studies suggest:
- 70–90% of people return to work within one year
- Some still report residual pain or reduced endurance
Real‑life example:
A construction worker in his 40s with a bicondylar fracture may return to work but need permanent modifications, such as reduced heavy lifting or more frequent breaks.
Overall prognosis and mortality
- 1‑year mortality after this injury is about 5%, especially in older adults with multiple health issues.
- This is why doctors pay close attention to your whole health, not just your knee.
Taking your medications, staying active within limits, eating well, and attending all follow‑ups protect both your leg and your life.

Frequently Asked Questions (FAQs) ❓
1. How long does it take to walk normally after a tibial plateau fracture?
Most people use crutches or a walker for 6–12 weeks, sometimes longer. Transition to normal walking often happens between 3–6 months, depending on fracture type, surgery, age, and rehab. Full recovery of strength and confidence can take 6–12 months or more.
2. Will my knee ever feel “normal” again?
Many patients regain excellent function, but some notice mild differences. You may feel occasional stiffness in the morning, discomfort on stairs, or weather‑related aches. Good alignment, strong muscles, and ongoing activity can make these issues minimal for many people.
3. Can I return to sports after a tibial plateau fracture?
Often yes, especially for low‑impact sports like cycling, swimming, or walking. High‑impact sports (running, basketball, singles tennis) are more variable. Decisions depend on imaging, strength, ROM, and your surgeon’s assessment. A gradual, supervised return is essential.
4. Do all tibial plateau fractures need surgery?
No. Stable, minimally displaced fractures can be treated nonoperatively with bracing or casting and careful follow‑up. Surgery is more likely if the joint surface is depressed, widened, unstable, or involves both sides of the plateau, or if you are active and need high function.
5. How can I reduce my risk of arthritis later?
You can help by:
- Staying at a healthy weight
- Keeping thigh and hip muscles strong
- Avoiding smoking
- Managing other joint conditions early
- Following your therapy plan and protecting joint alignment
Regular follow‑up with your orthopaedic surgeon helps catch changes early.
6. When should I worry about swelling and pain?
Mild swelling and aching are common for months. Seek urgent care if you have:
- Sudden, severe increase in pain
- New numbness, tingling, or cold foot
- Red, hot, very swollen calf
- Fever with a red, draining incision
These can signal compartment syndrome, DVT, or infection and need immediate evaluation.
Conclusion: Building a Strong Recovery After a Tibial Plateau Fracture 🌟
Healing from a tibial plateau fracture is a complex, step‑by‑step process. You are not just waiting for bone to mend. You are protecting cartilage, ligaments, and soft tissues, while slowly rebuilding strength, motion, and confidence.
To recap the five essential tips:
- Understand your injury and anatomy so the plan makes sense.
- Get accurate imaging and a tailored treatment strategy.
- Protect the repair while staying safely active.
- Commit to structured, honest, and consistent rehabilitation.
- Watch for complications and think long term about joint health.
Stay engaged with your surgical and rehabilitation team. Ask questions, speak up about concerns, and celebrate small gains. With patience, informed decisions, and steady effort, you give yourself the best chance for a stable, useful, and dependable knee in the years ahead. 💙
